About Angelman Syndrome
Testing 101
For a broad overview of genetic testing in AS, click here.
Angelman syndrome (AS) is always caused by a lack of functional UBE3A protein in the brain. Because there are different genetic causes, also called genotypes, for the lack of UBE3A protein, testing for AS can be very complicated! It can be frustrating and overwhelming, as it can take multiple tests and many months to get to the diagnosis and genotype. If you have questions about your loved one’s genetic testing (or your own!), please schedule with FAST’s board certified genetic counselor by clicking here.

Getting to a diagnosis of Angelman syndrome
In some instances, health care providers have a strong suspicion that an individual is living with AS, so that provider may recommend genetic testing specifically for AS. The flow chart below shows the typical testing process when AS is suspected.
In other cases, the health care provider may be unsure which disorder an individual might have and may start with a genetic test that looks for many different conditions at once. To learn more about genetic tests like chromosomal microarray or whole exome sequencing, click here.
Diagnostic testing for Angelman syndrome (when AS is strongly suspected).
^MS-MLPA can check methylation and test for deletion AS and ICD deletions in one test.
*Not all CMAs can detect UPD.
+Equals positive result.
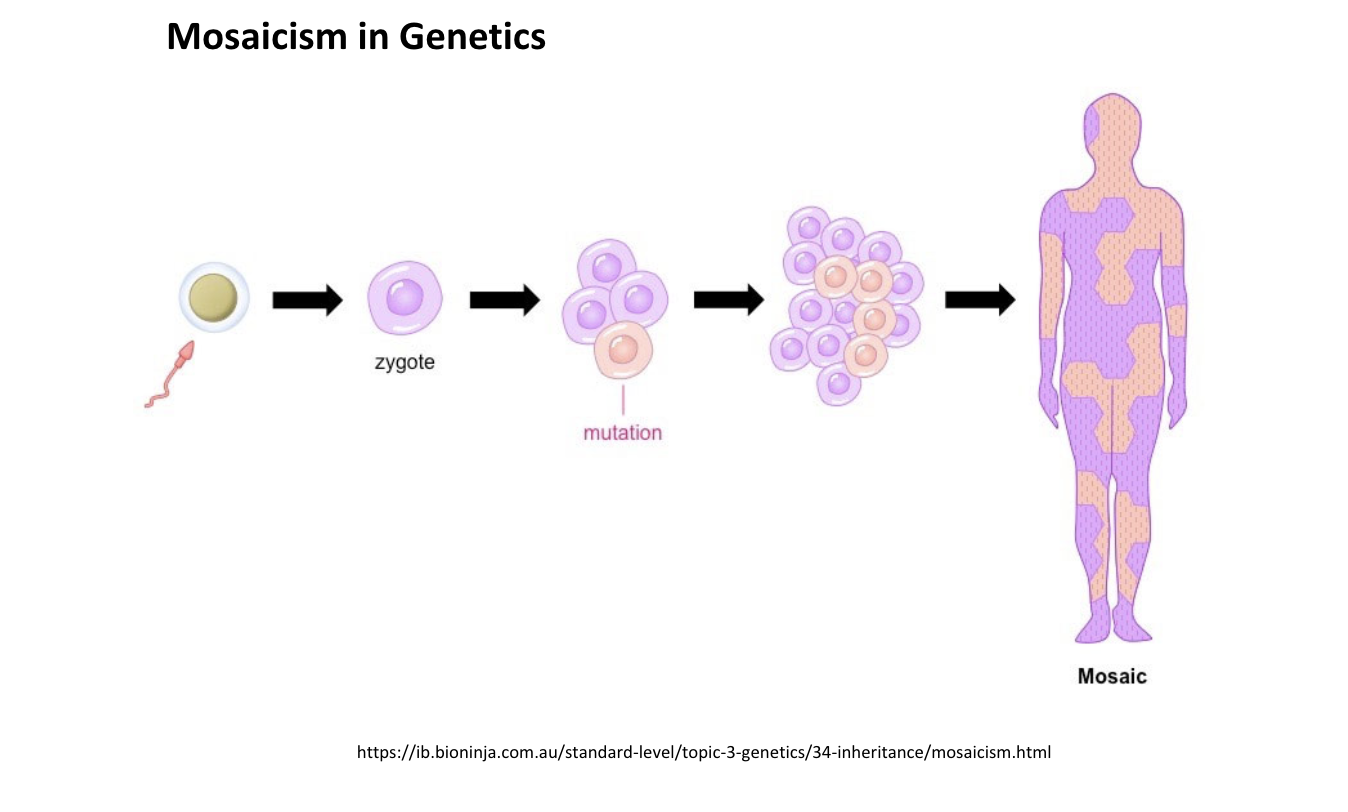
Mosaic AS does not have a specific test and can be identified on sequencing or methylation.

DNA Methylation testing is often the first step in genetic testing for Angelman syndrome. This test confirms the diagnosis of AS but does not determine the genotype.
If an individual is suspected to be living with AS, the first test that is typically performed is to look at the methylation on chromosome 15 in the region of the UBE3A gene. Methylation is a common mechanism in our cells to turn genes off and on. This region on chromosome 15 is imprinted, or expressed differently when inherited from the sperm (paternal) and from the egg (maternal) using methylation. Genetic laboratories can test for the methylation patterns in a person’s cells, typically on either blood or cells from a buccal (cheek swab) or saliva sample, to verify that both the maternal and paternal section of that chromosome region are present. Individuals living with AS who have a deletion, ICD, or UPD show a difference in their DNA methylation testing, with the maternal section appearing to be absent, which confirms the diagnosis of AS.
There are several different methods to test DNA methylation. Specific names of tests that can be ordered include: Southern hybridization methylation specific PCR (MS-PCR), methylation‐sensitive high‐resolution melting (MS-HRM), and methylation-sensitive multiplex ligation-dependent probe amplification (MS-MLPA).
If the methylation pattern confirms the diagnosis of AS, the next step is to determine the genetic cause, also called the genotype. Knowing the genotype is important because different genotypes are associated with different characteristics in the person living with AS and different chances for the family to have a future child with AS. In addition, clinical trials may have specific rules regarding which genotypes can enroll.
Identifying Mutation AS
Mutation AS cannot be identified on DNA methylation testing, because individuals living with Mutation AS have typical maternal and paternal methylation. Instead, they have a difference within the sequence of the UBE3A gene, which requires a different type of genetic testing called sequencing to identify. More information on sequencing is provided below.
For more information on each genotype, click here.

Methods to Determine AS Genotype
Deletion Testing
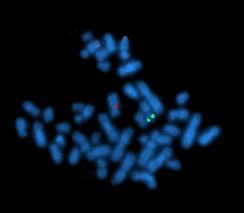
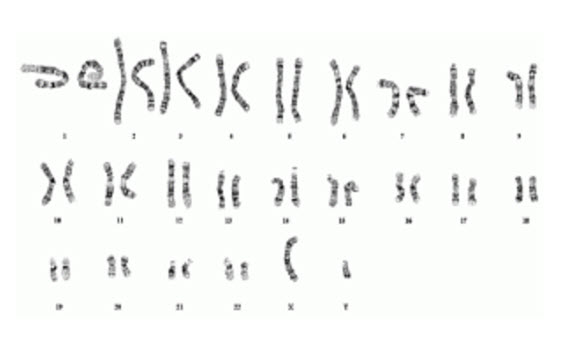
Because deletions are the most common cause of AS, testing for a deletion is typically performed next. This can be performed by many different methods, including fluorescence in situ hybridization (FISH), MLPA, or chromosomal microarray (CMA, also sometimes called comparative genomic hybridization or CGH or just array). One type of CMA (specifically SNP arrays or SNP-CMA) can also detect one type of UPD.

FISH was one of the first tests used for AS, and it is very accurate at determining whether an individual has a deletion in a very specific location. However, it cannot determine the size of the deletion, which can be helpful information in caring for a person living with AS. CMA and MLPA can more specifically determine where a deletion starts and ends, so they are now more commonly used to confirm deletions. MLPA can usually identify the typical AS deletions as well as ICD deletions.
Some labs perform MS-MLPA. MS-MLPA analyzes the methylation and looks for a typical AS deletion or an ICD deletion at the same time. You can think of it like a two-in-one test for AS, since it does both methylation and deletion testing at the same time.
UPD Testing
If methylation is consistent with AS and deletion testing does not show a chromosome 15q11.2-13 deletion, the next step is often to check for UPD. SNP-CMA can detect one type of UPD called isodisomy, which means that the two chromosome 15s from the sperm (paternal) are identical. The other type of UPD, called heterodisomy, happens when a person has two different chromosome 15s from the sperm. Isodisomy seems to be more common in AS. The type of UPD does not affect which symptoms or characteristics of AS an individual has. However, it can affect the ability to get diagnosed, since some tests can only detect isodisomy. A specific UPD test, usually just called UPD testing or UPD15 testing, may be used to check for heterodisomy. The UPD testing can identify both types of UPD and typically requires samples from both parents. UPD can also be identified on trio whole exome or trio whole genome sequencing, which again requires samples from both parents.

Imprinting Center Defect Testing
When the methylation is consistent with AS and deletion and UPD testing do not show the cause of AS, an individual is assumed to have an Imprinting Center defect (ICD). If ICD deletion AS testing was not already performed, that should be performed. If ICD deletion testing also did not find the cause of AS, most times the individual is assumed to have ICD Non-deletion.

{kind=link}
Mutation Testing (Typically referred to as UBE3A sequencing)
If the DNA methylation studies do not show an AS pattern and AS is still suspected, UBE3A sequencing is typically performed. The UBE3A gene is made up of nucleotides (the DNA chemicals) that provide the instruction for the UBE3A protein. The chemicals need to be arranged in a particular order for the protein to be made correctly. UBE3A sequencing looks at all of the nucleotides in the UBE3A gene, looking for any differences from the typical functioning UBE3A gene. Some individuals only have sequencing for the UBE3A gene, while other individuals will have sequencing for a panel of genes that includes UBE3A and other genes that may cause similar characteristics. Some individuals have sequencing of almost all of their genes through whole genome sequencing (WGS) or whole exome sequencing (WES).
Current sequencing results will report genetic variants that are pathogenic or likely pathogenic, meaning that the variant in the gene is either known to cause the condition or very likely to cause the condition. A pathogenic or likely pathogenic variant in UBE3A confirms the diagnosis of AS. This is often referred to as Mutation AS.
Sequencing reports will also include any variants of uncertain significance, sometimes called VUS or VOUS. VUS are differences from the typical gene sequence, but it is not clear whether the difference affects the function of the protein. VUS results can be tricky–in some cases a variant is called a VUS but it harms the UBE3A protein enough to cause AS; in other cases the VUS is just a random, harmless genetic difference. Family testing is often offered to try to better understand the VUS. If an individual has genetic testing for multiple genes, like in a panel or whole exome or genome sequencing, it is very common for the laboratory to find one or more VUSs in one of the genes that was tested.

{kind=link}
{kind=link}